 |
 |
|
 |
 |
About Us | Contact |
|
|
24/01/2007 - Study finds a 39% increase in brain tumours from mobile phonesThe latest Interphone study was surprisingly not press released, especially considering that they found a statistically significant increase in malignant brain tumours on the side of the head that the phone is used. This finding was for users that had first used their phone over 10 years ago, but considering the fact that only 77 of the cases in the study entered this category and the typical latency of a glioma is 15-25 years (diagnosis time after initial exposure), to find anything at all is quite remarkable, and highly likely to be the tip of the iceberg. The significant result is even more remarkable in the face of the flaw that we have previously commented on with the INTERPHONE study metric, where DECT phone exposure has been deliberately excluded from analysis. It was excluded on the basis that "they were not regarded as potential material exposure sources, since the average power that they transmit is only 0.01 W vs 0.25/0.125 W with GSM 900/1800 phones" (Data Collection para 1). Firstly, without any evidence to suggest that the effect has some kind of dose response relationship with the power level (which is unavailable due to the causal mechanism being unknown), this is poor scientific reasoning. It is also largely irrelevant now as there is peer-reviewed research demonstrating a similar effect (Increase in risk of all CNS tumours of 90% (CI 1.2-2.9)) from DECT phone usage [Hardell 2006]. If the link is found to be true, then (depending on the prevalence of DECT phones in the countries analysed) this could greatly dilute the effects found. There is also the now infamous protective effect that was found so strongly in the Danish study which we covered in December 2006. This is even more remarkable in this latest study: Table III in the study compares frequency of usage to non-users on a number of categories: Years since first use, Lifetime years of use, Cumulative number of calls, Cumulative hours of use, Cumulative number of calls by time since first use, and Cumulative hours of use by time since first use. These six categories split the data into 4 points: non-regular users (always with an OR as 1.0 as a control), and three degrees of severity in the regular user categories, which gives 18 points of data for regular users. To demonstrate our argument, we will separate the data into the lower two degrees of severity and the top degree of severity. Of the 12 less severe points (but still "regular" phone users), 11 out of 12 (91.67%) found a fully statistically significantly protective result - This result is astonishingly powerful, and should have been commented on strongly in the abstract if it was suspected to be real. By contrast, the 6 points in the most severe category are non-significant, but are, importantly, considerably higher in risk when compared to the less severe points. The following graph demonstrates the alarming trend quite appropriately, casting doubt on the protective effect found: 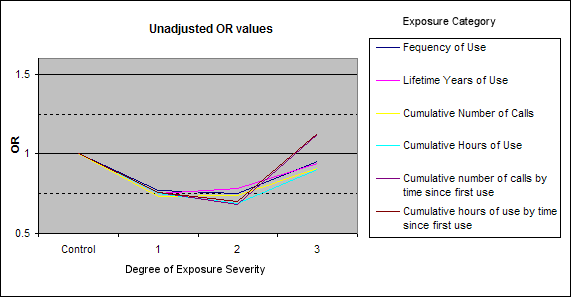 The unadjusted OR values show a striking and unexpected dip (protective), followed by a sharp rise for greater usage (protective effect disappears) Interestingly (and non-scientifically), I have also attached a graph where the less usage points have been adjusted to have an OR of approximately 1.0, to test what the data would represent if the drastic drop in OR was due to an inappropriate or inusuffiently well resolved exposure metric. It is clearly visible that if that was the case all of the most severe data points would find a statistically significant increase in malignant brain tumours: 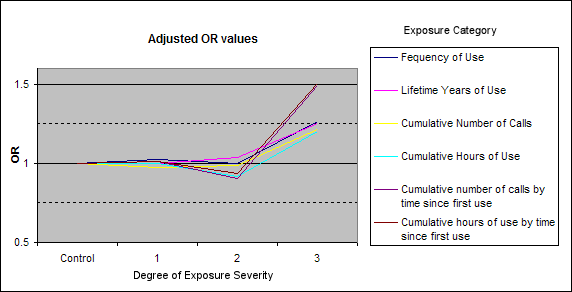 Of the most severe points, two are now fully statistically significant and three are marginally statistically significant, all for increased brain tumour risk So yet again an INTERPHONE study has data full of points showing a clearly protective effect of mobile phone usage in the vast majority of regular users that have not been using their phone for a prolonged period of time. They have not mentioned this in their abstract, nor have they postulated a reason as to why this could be. Not only that, but the protective effect disappears with more regular usage, implying that more regular usage is more harmful than less regular usage, which is protective when compared to no usage. This seems to make no sense, and would imply that there is an error in the exposure metric that is lowering the OR values for all regular users. If that is the case and the increase after 10 years is real, we can expect to see a far greater increase in another 5 years or so, when brain cancers would typically first expect to be seen. Links:[Lahkola A et al (2007) - Mobile phone use and risk of glioma in 5 North European countries] |

